5. Summary and Conclusions
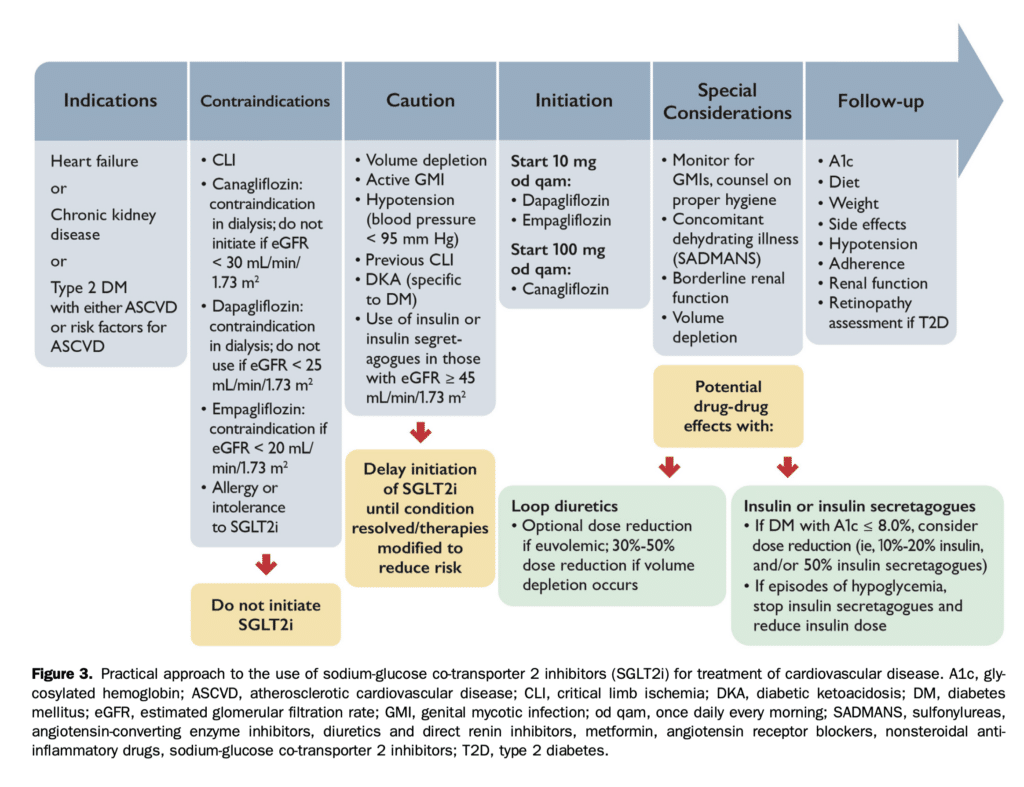
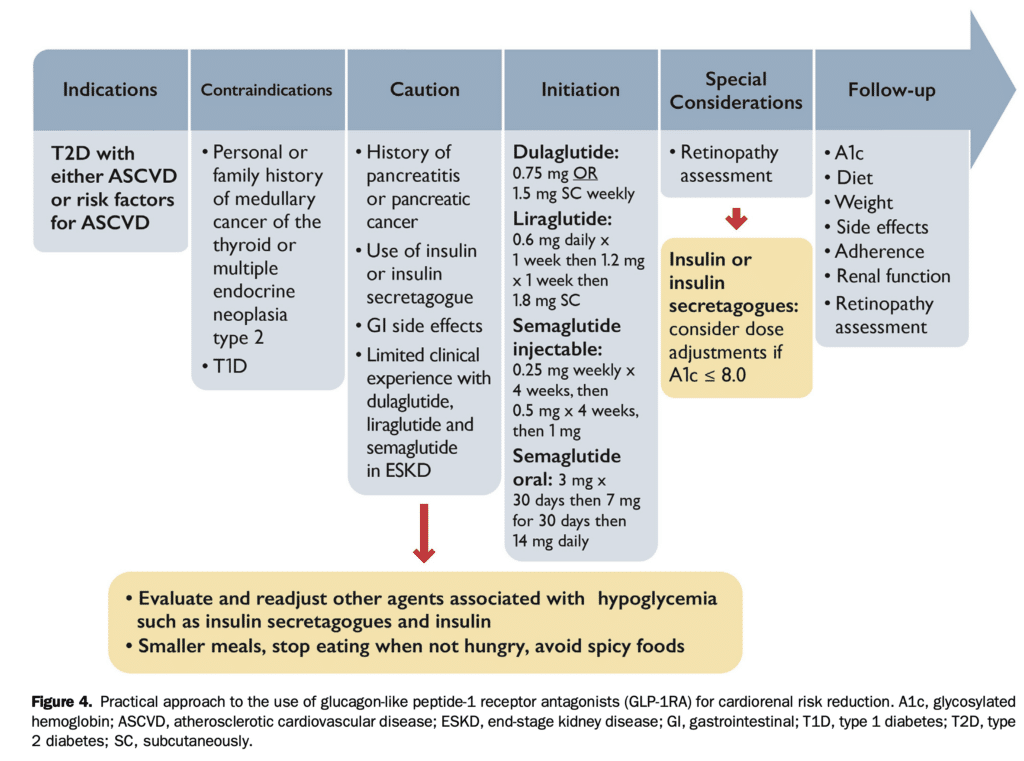
A remarkable paradigm shift has occurred with the availability of diabetes-related drugs with proven cardiorenal benefits in patients with and without T2D. We summarize our overview for appropriate, safe, and effective use of SGLT2i in Figure 3 and for GLP-1RA in Figure 4. CV medicine continues to progress with numerous new interventions shown to be clearly superior to historical standards of care and requiring practitioners to balance the proven benefits with administrative, economic, and access issues. These factors can complicate physician-patient decisions in the early stages of implementation but ultimately, evidence shows that more general incorporation of these treatments in appropriate patients will alter the natural course of disease. Achieving A1c targets continues to be an important goal for T2D. Also critical is the expeditious reduction of cardiorenal risk, thereby mandating a paradigm shift in prioritization of therapies. The profound benefits noted in the treatment of established HF or CKD or in the prevention of cardiorenal morbidity or mortality are not strongly tied to A1c-lowering. Accordingly, their initiation should not be predicated on the need for additional A1c-lowering. While upholding the principle of judicious stewardship of healthcare resources, it is imperative to advocate for lowering all hurdles to access of these classes of agents. Accordingly, the recommendations put forward can be considered ideal and aspirational, requiring tailoring to the specific and changing clinical environment faced by individuals with T2D, CKD, or HF and their healthcare professionals. This will require shared decision-making with the patient that reflects interdisciplinary collaboration from cardiologists, nephrologists, endocrinologists, primary care physicians, and pharmacists who should make every effort to integrate these diabetes-related agents with cardiorenal benefits into an overall and individualized treatment plan.
Supplementary Material
To access the supplementary material accompanying this article, visit the online version of the Canadian Journal of Cardiology at www.onlinecjc.ca and at https://doi.org/10. 1016/j.cjca.2022.04.029.